#036 – Eye Movement Technique on Executive Function and AFO + ES for Stroke
Estimated reading time: 4 minutes, 15 seconds.
Eye Movement Technique to Improve Executive Function in Patients With Stroke
A Randomized Controlled Trial 2021. (Open Access)
 Why
Why
- About 43–78% of patients will have cognitive dysfunction, including impairments of executive function (EF), thinking speed, and spatial orientation ability.
- 66.6% of the patients with stroke still had EF dysfunction 2 years after stroke, mainly at the levels of choice, planning, decision-making, and control behavior disorder in daily life.
- Stroke patients show a variety of eye movement disorders, including reduced saccade and difficulty retaining spatial position, which are caused by damage to the muscles outside the eye, the cranial nerves that supply the eye muscles, or the neural pathways that control them. Affecting 70% of stroke patients
- A reduced ability to scan the visual environment may affect visual memory, recognition, and the ability to make plans and decisions, affecting EF.
- The neurologic basis of eye training is to participate in the regulation of the vestibular reflex (VOR), which plays an important role in the perception of spatial position and balance of the human body.
- few studies have reported the efficacy of the combination of routine rehabilitation and eye movement technique on executive function in patients with stroke.
- Therefore, this study investigated an EF rehabilitation strategy based on routine rehabilitation combined with the eye movement technique.
 How
How
Participants and interventions groups:
- 32 Participant in intervetions group and 32 in control group.
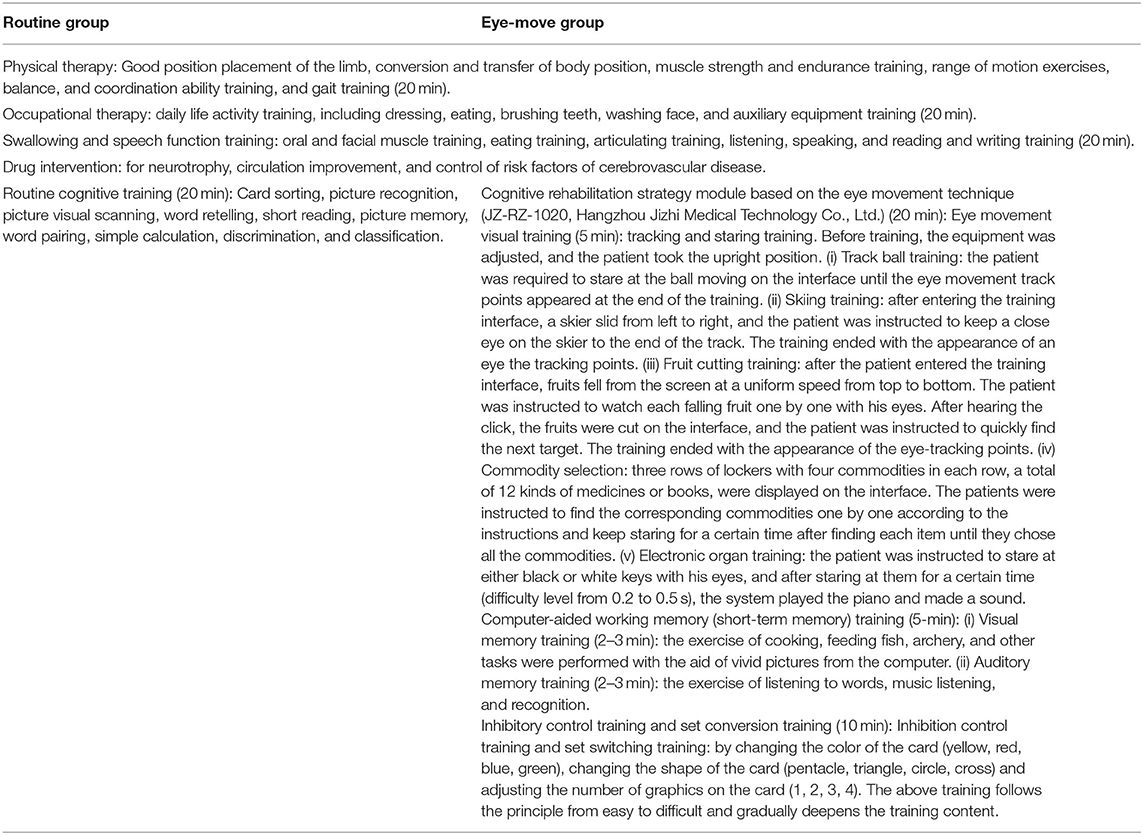
Detials of interventions here.
- The participants in the routine group received regular cognitive rehabilitation training, while the participants in the eye-move group received cognitive rehabilitation based on the eye movement technique.
- The rehabilitation intervention in the two groups was performed 6 days a week for 6 weeks.
- 7 to 10 weeks follow-up time.
Assessment methods:
- Self-Rating Depression Scale (SDS), Self-rating Anxiety Scale (SAS), Montreal cognitive assessment (MoCA), Behavioural assessment of the dysexecutive syndrome (BADS), Wisconsin Card Sorting Test (WCST), Reaction time test and modified Barthel Index (MBI).
 Results:
Results:
- The BADS dimensions and WSCT dimensions (except “number of categories completed”) were significantly improved in the eye-move group.
- The BADS score of the intervention group were significantly higher than those of the routine group, and other sub-scores of the WCST in all dimensions were better than those of the routine group except “learning to mastering.”
- Suggesting that eye movement techniques could effectively improve the EF of stroke patients.
- The response time of the two groups was significantly shortened and the MOCA score was significantly improved, and the improvement was more obvious in the eye-move group than in the routine group.
- Suggesting that eye movement technology can effectively improve the attention and cognitive function of the patients.
- The “rule switching card” in the BADS and the “correct response number,” “false response number,” and “persistent error number” in the WSCT were significantly improved after the intervention compared with the routine group.
- Suggesting that the improvement of these indicators is through the improvement of inhibitory control ability in EF.
- After 4 weeks of follow-up, the BADS, WSCT, and MOCA scores and response time of patients in both groups were decreased compared with those after the intervention.
- Suggesting that although the intervention lasted 6 weeks and achieved some results immediately after the intervention, the training time might not be enough to stabilize these changes.
 Conclusion
Conclusion
- This study indicates that rehabilitation training using the eye movement technique was beneficial to the recovery of EF and the improvement of quality of life in patients with stroke.
Ankle-Foot Orthoses and Functional Electrical Stimulation Post-Stroke
A Clinical Practice Guideline. 2021 (Resticted Access)
Results
- One-hundred twenty-two meta-analyses, systematic reviews, randomized controlled trials, and cohort studies were included.
- Strong evidence exists that AFO and FES can each increase gait speed, mobility, and dynamic balance.
- Moderate evidence exists that AFO and FES increase quality of life, walking endurance, and muscle activation, and weak evidence exists for improving gait kinematics.
- AFO or FES should not be used to decrease plantarflexor spasticity.
- Studies that directly compare AFO and FES do not indicate overall superiority of one over the other. But evidence suggests that AFO may lead to more compensatory effects while FES may lead to more therapeutic effects.
- Due to the potential for gains at any phase post-stroke, the most appropriate device for an individual may change, and reassessments should be completed to ensure the device is meeting the individual’s needs.
 Limitations
Limitations
- This CPG cannot address the effects of one type of AFO over another for the majority of outcomes, as studies used a variety of AFO types and rarely differentiated effects.
- The recommendations also do not address the severity of hemiparesis, and most studies included participants with varied baseline ambulation ability.
Also, in stroke
- The results of the meta-analysis, based on a limited number of studies, did not show significant superiority of computer-based cognitive training compared to the traditional method in post-stroke patients. (Restricted Access)
- The evidence for the effect of the PNF on spasticity in patients with stroke was limited. A systematic review (Restricted Access)
- Mirror therapy can improve edema, pain and functional activities in patients with post-stroke shoulder-hand syndrome. RCT (Restricted Access)
Thank you for reading, see you in the next one.

{kind=link}